

Blog
Hexarelin vs Ipamorelin: Key Differences for GHS Research
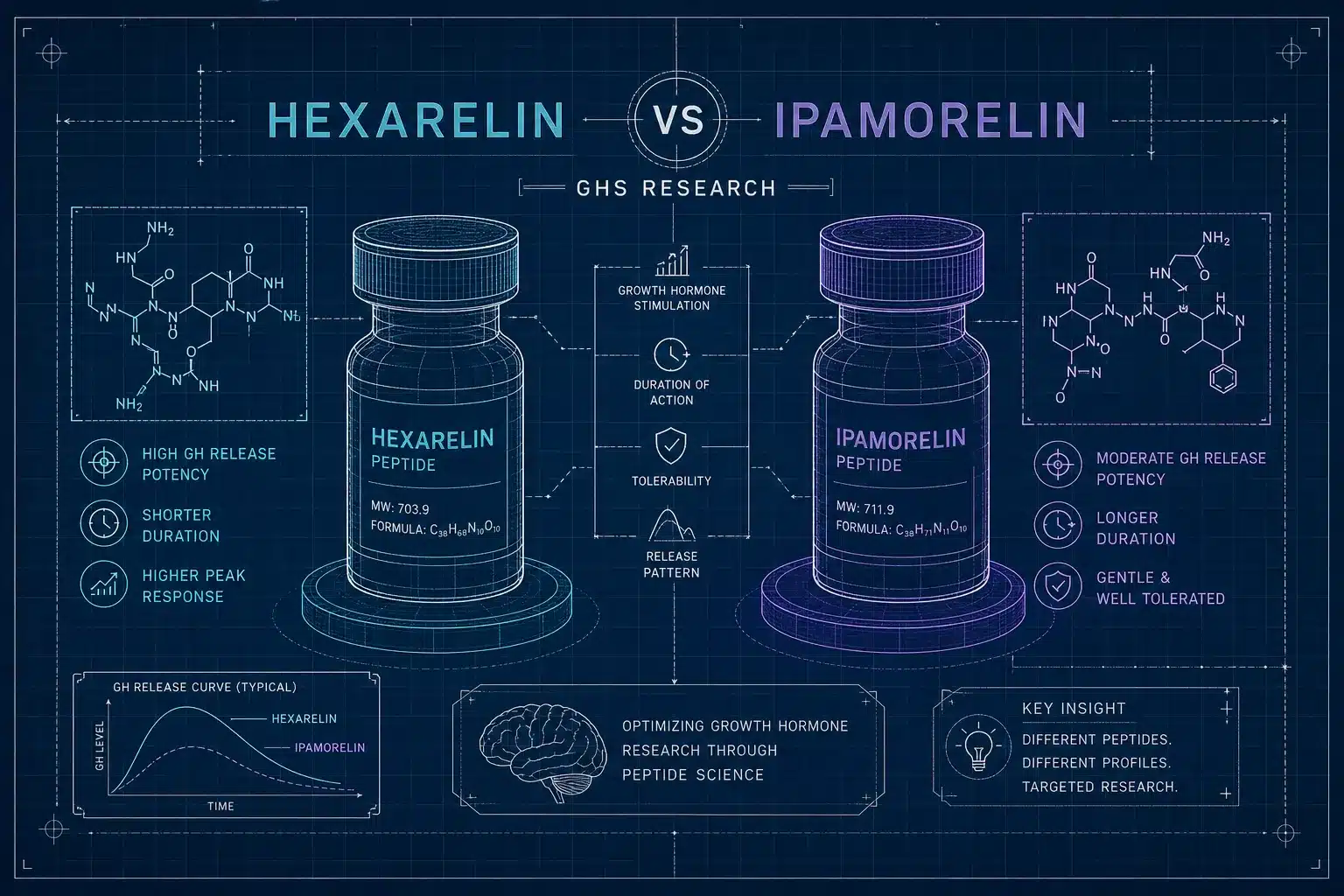
Understanding what is the difference between ipamorelin and hexarelin in growth hormone secretagogue research is not a trivial question. Both compounds activate the ghrelin receptor pathway and appear side by side in the same research catalogs. Treating them as interchangeable in a study design, however, is a methodological error that surfaces in data you cannot cleanly interpret. The structural differences between these two compounds produce distinct receptor profiles, separate hormonal footprints, and different tachyphylaxis patterns that directly determine what a study can and cannot measure.
This article breaks down the pharmacological, mechanistic, and endocrinological distinctions that matter most for researchers designing comparative GHS protocols. For labs and independent researchers running both compounds side by side, sourcing them from a single verified supplier with matched-lot COAs keeps the comparison clean. R-Peptide Supply (Grey Peptide Shop) carries both hexarelin and ipamorelin with full COA documentation and bulk-friendly vial formats, exactly the kind of setup worth having before a protocol begins.
Structural differences that shape their pharmacology
Hexarelin’s hexapeptide backbone
Hexarelin is a synthetic hexapeptide with the sequence His-D-2MeTrp-Ala-Trp-D-Phe-Lys-NH2, derived from the met-enkephalin sequence. The D-amino acid substitutions at specific positions were likely engineered to resist enzymatic degradation and improve receptor binding stability across biological compartments. Those same substitutions, however, open the door to off-target receptor interactions that shorter, more selective sequences do not produce. The compound’s structural breadth is both its strength and its experimental liability.
Ipamorelin’s pentapeptide design and selectivity intent
Ipamorelin is classified as a pentapeptide with a sequence incorporating an alpha-aminoisobutyric acid (Aib) residue at the N-terminus, contributing to its conformational stability and selectivity. It was developed specifically to eliminate the hormonal noise observed with earlier GHRPs, and its sequence was optimized in animal models to generate clean GH pulses without engaging corticotropic pathways. That design philosophy is embedded in the structure itself, not a downstream pharmacological coincidence. When ipamorelin produces a selective endocrine response, it is because the sequence was built to do exactly that.
Why sequence length and substitution matter experimentally
A compound with broader receptor contact points introduces more biological variables for the researcher to control. When hexarelin’s sequence creates conditions for off-target binding, every downstream measurement carries that complexity. Ipamorelin’s shorter, more constrained sequence reduces that surface area. The structural comparison sets up everything that follows in receptor binding and hormonal readout, and it is the first place to look when asking about the difference between ipamorelin and hexarelin in GHS research. For a focused methodological breakdown see the Ipamorelin vs Hexarelin: Which GH Secretagogue Wins?
Receptor binding profiles: what is the difference between ipamorelin and hexarelin in growth hormone secretagogue research
GHS-R1a agonism in both compounds
Both hexarelin and ipamorelin activate GHS-R1a, the canonical ghrelin receptor, which drives the GH-releasing effect in pituitary and hypothalamic tissue. Both engage intracellular calcium signaling downstream of GHS-R1a activation, producing the familiar GH secretory pulse. Hexarelin is reported to have high receptor affinity at GHS-R1a with strong agonist activity at this site, along with documented activity at secondary binding sites discussed below. That shared GHS-R1a mechanism is where the similarity largely ends.
Hexarelin’s off-target receptor footprint (CD36 and cardiac sites)
Hexarelin binds CD36, a scavenger receptor expressed in macrophages, endothelial cells, and cardiac tissue, with a measured cardiac binding Kd of approximately 14.5 nmol/L. Cardiac binding studies identified hexarelin receptor sites in heart tissue that are pharmacologically distinct from pituitary GHS-R1a sites, confirming a separate binding compartment rather than simple GHS-R1a spillover. The CD36 interaction is the mechanistic basis for hexarelin’s direct cardiovascular effects, and those effects operate independently of GH secretion. Researchers designing GH-focused studies who ignore this receptor footprint are working with an incomplete variable map.
Ipamorelin’s narrower receptor footprint
Selectivity studies, including a 1998 pig model study by Raun et al., frame ipamorelin as a highly selective GHS-R1a agonist with no strongly established off-target receptor comparable to hexarelin’s CD36 binding. Its selectivity is the core reason ipamorelin produces a cleaner endocrine readout in study designs focused purely on GH-axis activity. For protocols where the experimental question is GH secretion and nothing else, that narrower receptor footprint is a direct methodological advantage. See the original selectivity work and related analyses for context in the literature (Raun et al. and review).
GH release potency, onset, and half-life compared
Hexarelin’s documented GH potency and time-action profile
In healthy human volunteers given intravenous hexarelin boluses, GH release was dose-dependent and well-quantified. Peak plasma GH concentrations reached 26.9, 52.3, and 55.0 ng/mL at doses of 0.5, 1, and 2 µg/kg respectively, with GH peaking at approximately 30 minutes post-dose and returning to baseline by 240 minutes. The reported elimination half-life is approximately 55 minutes in humans and 75.9 ± 9.3 minutes in rats after IV dosing. Subcutaneous hexarelin in rodent models produced long-lasting GH release and slightly outperformed GHRP-6 in some comparative settings.
Ipamorelin’s GH profile and selectivity advantage
Ipamorelin produces pulsatile GH release with peak GH and AUC as the primary endpoints in published work. Primary human pharmacokinetic data report a terminal half-life of approximately 2 hours, with clearance of 0.078 L/h/kg and a steady-state volume of distribution of 0.22 L/kg. Plasma ipamorelin Cmax ranged from 30 to 809 nmol/L across doses, with corresponding GH Cmax values of 20 to 223 mU/L and GH AUC values of 30 to 373 mU·h/L. The key distinction from hexarelin is not raw GH magnitude but the clean endocrine background: ipamorelin’s GH signal arrives without the ACTH and cortisol noise that complicates interpretation in hexarelin studies.
Practical implications for study design
Hexarelin’s stronger acute GH pulse suits short-window potency experiments where maximal GH stimulation is the endpoint. Ipamorelin’s selective profile is the better instrument for studies where pituitary-adrenal crosstalk needs to be excluded as a confounding variable. Choosing between them is not a quality judgment; it is a question of matching compound pharmacology to experimental design. For additional comparative methodology and protocol recommendations, consult the researcher’s comparison guide.
Off-target hormonal effects and cardiovascular signals
Hexarelin’s ACTH, cortisol, and prolactin stimulation
Published human studies report that hexarelin stimulates prolactin, ACTH, and cortisol in addition to GH. The ACTH and cortisol-releasing activity has been described as comparable in magnitude to human CRH, and prolactin release, while lower than TRH-stimulated responses, is still measurable. For researchers focused on GH-axis-specific outcomes, this hormonal spillover creates confounding variables that require active management. Including baseline and post-dose panels for ACTH, cortisol, and prolactin is not optional in a rigorous hexarelin protocol, it is a minimum data requirement.
Ipamorelin’s clean hormonal profile
In the available studies, ipamorelin produced no statistically significant elevation in ACTH or cortisol in animal models at physiological research doses, and prolactin remained similarly unaffected. The 1998 Raun et al. selectivity study in pigs confirmed this profile specifically, and subsequent secondary literature consistently supports it. This makes ipamorelin the stronger instrument for protocols where the experimental endpoint is GH secretion independent of adrenal or corticotropic activation. The endocrine background remains suppressed, leaving the GH signal as the dominant readout.
Hexarelin’s cardiovascular effects and what they mean for study design
In isolated perfused rat heart preparations, hexarelin produced dose-dependent increases in coronary perfusion pressure, with coronary resistance reaching 11.0 ± 0.7 mm Hg·min/mL at 30 µmol/L and coronary perfusion pressure rising by up to 120%. These effects were blunted in CD36-deficient preparations, confirming receptor-mediated coronary vasoconstriction.
In intact human studies, hexarelin increased mean arterial pressure without affecting heart rate, improved LVEF and cardiac output, and reduced wedge pressure, demonstrating that in-vivo hemodynamic responses differ meaningfully from isolated-heart findings. Researchers running cardiovascular endpoints alongside GH measurements must account for hexarelin’s direct cardiac pharmacology as a separate variable from its pituitary-mediated GH release. No strong evidence to date supports similar cardiovascular confounds with ipamorelin, though dedicated cardiovascular-focused ipamorelin studies remain limited.
Tachyphylaxis in secretagogues: comparing ipamorelin and hexarelin in GHS studies
Hexarelin’s desensitization profile
Prolonged or repeated hexarelin administration is documented to reduce the acute GH response over time, consistent with classic secretagogue tachyphylaxis. Rodent data show that the pattern is age- and model-dependent: neonatal rats given hexarelin at 80 µg/kg twice daily for 3 to 10 days showed enhanced GH responses over time, while adult rats given 150 µg/kg twice daily for five days showed no such enhancement, suggesting adult-model attenuation rather than sensitization. Attenuation appears to track with continuous or high-frequency dosing, consistent with pulsatile receptor stimulation being protective against desensitization. Researchers running chronic hexarelin protocols should build washout periods into the design and plan primary endpoint measurements at fixed intervals early in the treatment window.
Ipamorelin’s relative stability with repeated dosing
Ipamorelin’s more selective GHS-R1a activation is generally associated with a more stable repeated-dose GH response compared to older, less selective GHRPs. Current literature does not document the same degree of tachyphylaxis with ipamorelin that appears in hexarelin and GHRP-2 studies, though the comparative evidence base for long-duration ipamorelin protocols remains smaller. That relative stability makes ipamorelin more tractable for longer-duration experimental timelines where maintaining consistent GH pulse amplitude is part of the study design.
Dosing cadence strategies for multi-week GHS protocols
General GHS pharmacology supports avoiding continuous receptor stimulation to preserve response amplitude: pulsatile dosing schedules consistently outperform continuous infusion in maintaining GH output, and this principle applies across the secretagogue class. For comparative studies running both compounds simultaneously, aligning dosing intervals and washout windows is essential to produce interpretable cross-compound data. Without synchronized cadence design, differences in tachyphylaxis rate between hexarelin and ipamorelin will confound any side-by-side GH comparison.
Sourcing hexarelin and ipamorelin for comparative GHS research
Why matched-lot sourcing matters in comparative studies
When running a hexarelin vs. ipamorelin head-to-head protocol, using compounds from the same supplier and the same verification batch eliminates one additional variable from the comparison: lot-to-lot purity variation. A COA with HPLC purity data for each peptide should be reviewed before any dosing protocol begins. Without that documentation, concentration assumptions entering the study are unreliable, and observed differences between compounds could reflect purity variance rather than genuine pharmacological divergence.
Consolidating both compounds through a single verified supplier
R-Peptide Supply (Grey Peptide Shop) carries both hexarelin and ipamorelin with verified COAs available for each lot, in multi-vial bulk formats suited to extended research protocols. Having both peptides sourced from the same supplier with matched documentation reduces pre-study administrative friction and keeps the comparison foundation solid before the first vial is prepared. All products are sold for research use only. For ordering details and bulk pricing, see how to buy ipamorelin and hexarelin online.
Choosing the right tool for the research question
The clearest way to summarize the difference between ipamorelin and hexarelin in GHS research: hexarelin is the higher-potency, broader-receptor compound with documented cardiovascular activity, corticotropic stimulation, and CD36 binding that extend well beyond the GH axis. Ipamorelin is the cleaner, more selective GHS-R1a agonist that delivers a stable, interpretable GH signal without adrenal or cardiac confounds. What separates these two peptides in growth hormone secretagogue research ultimately comes down to what the study is measuring and which variables the researcher can afford to leave uncontrolled.
If the endpoint is raw GH stimulation and the cardiovascular or adrenal context is itself part of the research question, hexarelin provides more variables to study and quantify. If the goal is an isolated, interpretable GH-axis response with minimal hormonal noise, ipamorelin reduces that background and lets the GH signal speak clearly. Neither answer is universally correct; the compound has to match the experimental question.
Researchers who understand these distinctions can design tighter protocols, anticipate confounding signals, and interpret results with greater confidence. Building that comparison on verified, COA-documented compounds from a single wholesale source like R-Peptide Supply means the methodological foundation is solid before any data is collected, and a rigorous GHS research design always starts with that foundation.
For an alternate practical comparison and additional notes on experimental endpoints, consult our full Ipamorelin vs Hexarelin: A Researcher’s Comparison Guide.